Posterior STEMI Bypass
Question# 752
Answer:
Hello and thank you for your MedicASK regarding posterior STEMI bypass.
To answer your question in short, yes, you would transport to the heart institute on a bypass for a posterior STEMI. Here is a deeper look into this type of STEMI which you may find helpful in your practice moving forward.
Posterior infarction accompanies 15-20% of STEMIs, and is typically seen alongside an inferior or lateral infarction. To have an isolated posterior MI is rare and only seen in approximately 3-11% of patients with infarcts. This is indicative of emergent coronary reperfusion meaning, the patient requires a PCI centre. In order to truly determine if your patient is having a posterior STEMI, a 15-lead must be performed which requires movement of leads V4, V5, and V6, which we will review more in a minute. That said, the lack of obviousness on a standard 12-lead ECG means the diagnosis is unfortunately often missed leading to delays in treatment.
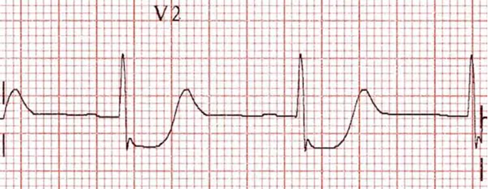
So how do we suspect if a patient is having a posterior STEMI utilizing a standard 12-lead, in order to determine if a 15-lead is needed? The answer is to be vigilant in patients who are presenting with either an inferior or lateral STEMI. When looking at V1-V3, the following changes are suggestive of a posterior MI:
- Horizontal ST depression
- Tall broad R waves
- Upright T waves
- Dominant R waves in V2 as seen in the picture below:
The simple explanation of why we see this is due to the posterior electrical activity being traced from the anterior side of the heart, which causes the typical injury pattern of ST elevation and Q waves to become inverted:
- ST elevation actually becomes ST depression
- Q waves become R waves
- Terminal T-wave inversion becomes an upright T-wave
So if you were to see these changes on a 12-lead ECG and you were to flip it upside down, you would then see this instead:
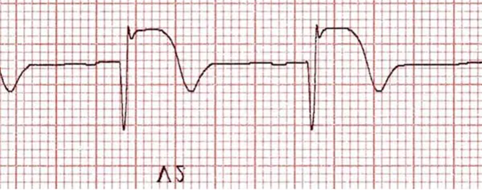
Wow right?! We would not hesitate take this patient on a STEMI bypass!!!
Because we don’t do 15-leads often, below is a quick review of proper lead placement. There are two ways of completing a 15-lead (both are correct):
1.) This 15-lead is what is outlined in the Companion Document (p. 9) and is the one we would typically do in the pre-hospital setting as we are already moving V4 to V4R (modified 15-lead/minimum expectation) for inferior STEMI's, to rule out a right ventricular infarct when considering nitroglycerin. This version saves you an extra lead movement as you should already have a high index of suspicion of a posterior MI with inferior ST elevation as mentioned above:
V4=V4R, V5=V8, V6=V9
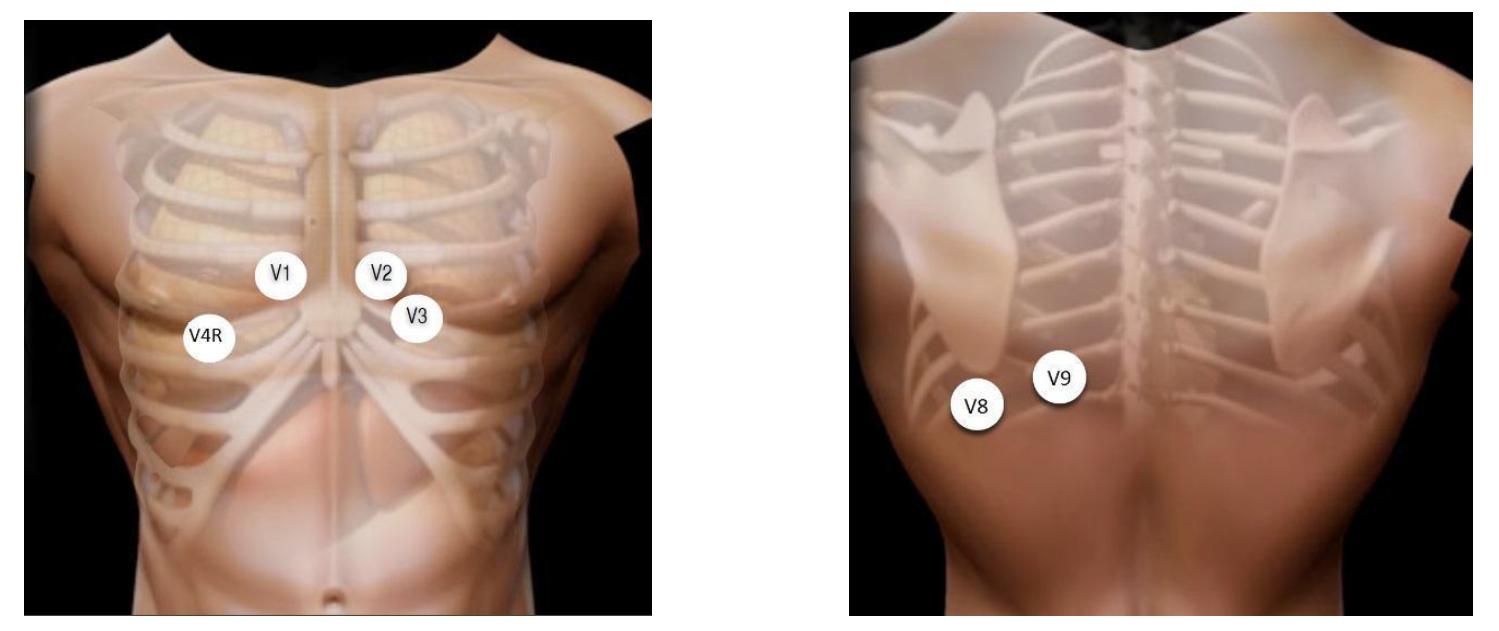
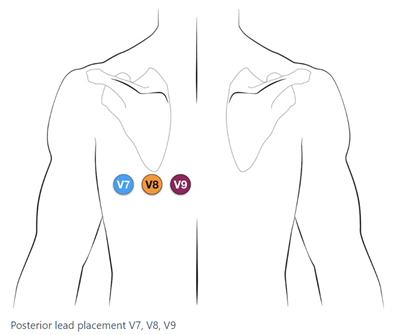
2.) This 15-lead is typically done in the hospital setting:
- V4=V7 – Left posterior axillary line, in the same horizontal plane as V6
- V5=V8 – Tip of the left scapula, in the same horizontal plane as V6
- V6=V9 – Left paraspinal region, in the same horizontal plane as V6
Remember to always write these changes on the ECG printout for the receiving hospital along with the patient's name and DOB, and to also document in your ePCR the time at which the 12-lead becomes a 15-lead with the changes/new leads.
In comparison to the 1-2 mm of ST elevation that we are used to, it actually only takes 0.5 mm of ST elevation to make a posterior MI diagnosis because this patient is critical. Posterior MI’s are often the result of an occluded nondominant circumflex artery.
MI’s affecting the posterior wall frequently do not meet STEMI criteria which requires the paramedic to use interpretation skills above and beyond the current guidelines. A 15-lead ECG is not mandatory and should not delay treatment/transportation however, if time permits it can be a useful tool in assisting with your diagnosis.
Marked ST elevation in V7-V9 with the presence of Q-wave formation indicates posterior wall involvement. This ECG depicts an inferior-lateral-posterior STEMI:
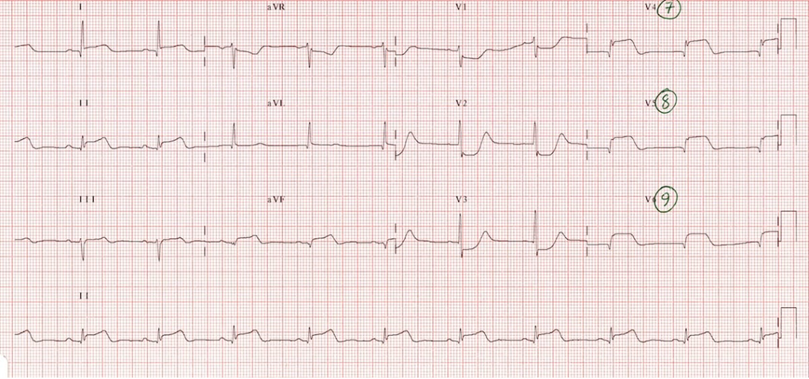
This suggests a much larger area of myocardial damage and these patients are at a much greater risk of ventricular arrhythmias and death. This once again highlights why it is crucial and that the expectation is to have the pads placed on all STEMI patients. As you stated, this patient would still be treated as any other cardiac ischemic STEMI patient provided they don't have any contraindications.
Here is another useful pneumonic you can use to assist with determining STEMI’s when assessing for reciprocal changes (ischemia) in the field:

Hope this helps clarify your question! Please don't hesitate to reach out should you have an additional questions or concerns!
References
chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://ontariobasehospitalgroup.ca/wp-content/uploads/2023/03/2023-02-01_v5.1_Companion-Document.pdf
https://litfl.com/posterior-myocardial-infarction-ecg-library/
https://litfl.com/ecg-lead-positioning/
https://www.ncbi.nlm.nih.gov/books/NBK553168/