
Read more …Data Request for Research Form
- Hits: 5503
Read more …Data Request for Research Form


Both de-activation and de-certification signify a stop in a paramedic's authorization from the Medical Director to perform controlled medical acts. Whether de-activated or de-certified, the paramedic is no longer eligible to work as a paramedic within the certifying base hospital, except in the case of a partial clinical de-activation (see below). De-activation and de-certification may be the result of several different processes outlined below.
Most administrative de-activations are due to a paramedic's absence from work for periods greater then 90 days. After ninety days away from practice, paramedics are required to undertake a Return to Clinical Practice process and are deactivated until that process is complete. Following completion of a Return to Clinical Practice process, the RPPEO reactivates paramedics' certification.
Other potential reasons for administrative de-activation include failure to complete annual maintenance of certification activities by the deadline or failing to respond to RPPEO requests for information during audits. It's also used when the RPPEO anticipates that a paramedic plans to continue practising within the RPPEO region, but is missing some aspect of their administrative file in order to continue. In these rare cases of missing information, administrative de-activation can almost always be reversed by providing the missing administrative details.
When the Medical Director has serious concerns about the safety and quality of clinical care, they may use clinical de-activiation to limit a paramedic's activity. In the case of a full clinical de-activation, the Medical Director removes a paramedic from all clinical activities, while a partial de-activation means removing authorization for certain specified clinical activities. Following investigation of the issues, paramedics may be required to undergo remediation or other educational activities to have their certification re-reactivated. While the RPPEO maintains this process should it be required, de-activation for concerns about patient care or safety is exceedingly rare.
The RPPEO de-certifies paramedics who have left our region or who are retired from practice. There is a Ministry of Health mechanism for de-certification on the basis of patient safety concerns described in Appendix 6 of the Advanced Life Support Patient Care Standards, however, clinical decertification is extremely rare. When it does occur, it's at the recommendations of a Paramedic Practice Review Committee (PPRC). By the PPRC's review and recommendation, a paramedic who no longer meets the requirements set out in the provincial Patient Care Standards, the RPPEO's policies and/or other requirements of the Ministry of Health will be de-certified. The authorization to practice as a paramedic under the jurisdiction of the base hospital and the authorization to perform delegated controlled medical acts are thereby withdrawn.
For more details about de-activation and de-certification, see the RPPEO Certification Policy.

No one wants an administrative deactivation, but that's what the automation bot working inside MedicNET does on February 1 if you're missing requirements.
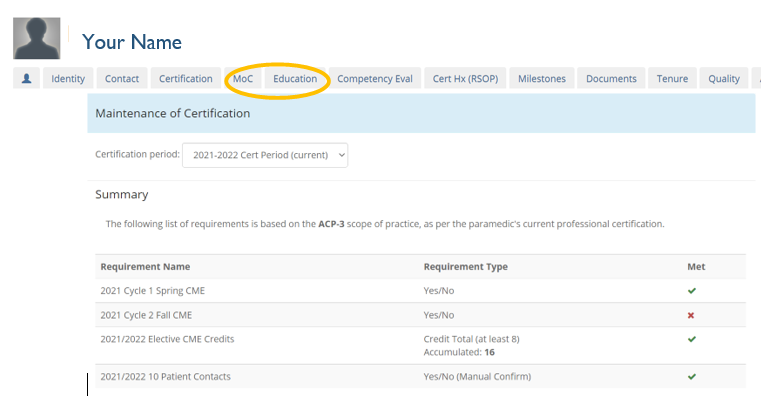
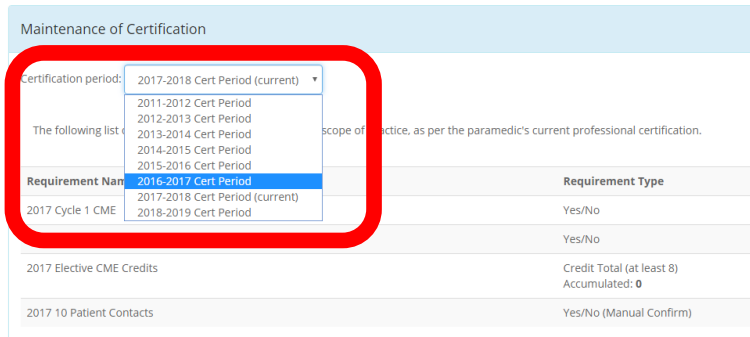
If you're in the group with administrative deactivation, check your MedicNET profile to see what you're missing. Read the FAQ below to find out how to proceed when you're ready for your paramedic certification to be re-activated.
The humans at the RPPEO are always happy to hear from you! For more about your annual CME requirements or other recertification issues, contact us at certification@rppeo.ca or 877-587-7736.
For those who have successfully re-certified for the current year, congratulations and thank you!

Go to MedicNET
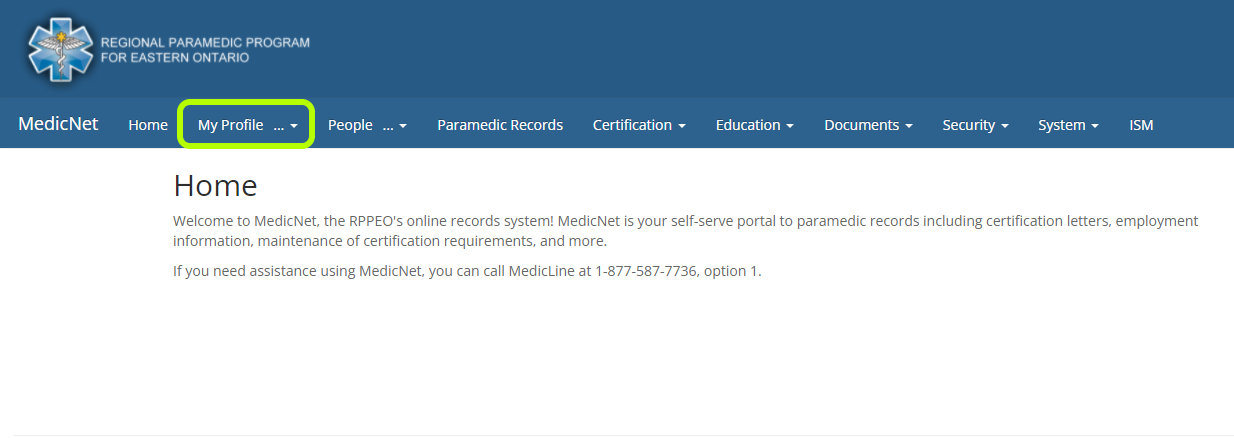
Just below your name
A. January 31, each year at 23:59:59.
A: The requirements are detailed by scope of practice in the RPPEO’s Certification Policy CERT 100 available here.
A: Please log into our website and view your profile in MedicNET (see instructions)
A. An online course is available in MedicLEARN as an approved alternative.
Title of the course: 202x-202x MOC 10 Patient Contacts Equivalency.
Direct link to MedicLEARN: 10 Patient Equivalency Course
A. You can email us at certification@rppeo.ca or call MedicLINE at 1-877-587-7736 Option 1.
A. The system will issue you an administrative deactivation letter.
A. Simply complete the missing requirement(s) online as soon as possible. Once all requirements are met, RPPEO will reactivate you.
{rseventspro type="upcoming"}
Read more …Education Events List

Read more …Elective CME Pre-Approval Request

Thank you for completing this Online Learning Module using the RPPEO's E-Learning Portal. If you have any questions, comments or concerns please direct them to certification@rppeo.ca
We hope you have enjoyed this part of the process and welcome any feedback on what we can improve upon.
RPPEO Certification Team
Q - What are aliquots and when should you use them?
A - Small, equal parts of the maximum single dose that are administered q 3 minutes until the desired analgesia is achieved or the maximum single dose is reached. Paramedics should document the total amount of a single dose administered and not each individual aliquot as a separate dose.
Q - What are the differences between opiate naïve and opiate tolerant? And why is this important in dose preparations?
A - o An opiate naive individual is someone who has not taken opioids regularly or recently enough to develop tolerance. This can include people who have never used opioids or those who have not used them for a significant period, often defined as 7 to 120 days, depending on clinical guidelines. Because their bodies have not adapted to opioids, even a small dose can produce a strong effect.
Q - Which analgesia option is best?
A - Paramedics are encouraged to use their clinical judgment when choosing which analgesia is best suited for their patient.
Q - How do I choose between using an opioid and ketamine?
A - Clinical judgement should include weighing the risks and benefits of using the various medications. This includes: previous use, other medications the patient is taking, medical history, event history, current and expected hemodynamic stability.
Q - What are the main methods to monitor patients that have received opioids, benzos, or ketamine?
A - EtCO2, RR, HR, BP, LOA, O2 sats, signs of adverse reactions.
Q - Can you start dosing at lower amounts than what is written in the medical directives?
A - Yes, it is appropriate to consider utilizing a lower dosing regimen set out in the ALS PCS. Aliquots are also useful in these situations. Paramedics are encouraged to use clinical judgement to promote patient safety. Document all reasoning on ePCR. If unsure, patch to a BHP.
Q - When Palliative first came out there was discussion around increased “breakthrough” dosing of +10% of the patient’s regular dose. Is this something we are still doing and can patch for?
A - Currently it is recommended to stick with the current dosing regimen of 0.5mg-2mg. The recommendation is to stick with these standard doses, reassess, and titrate if required.
Q - With some services getting Methoxyflurane, what is the recommendation on using it concurrently with opiates and ketamine?
A - As with other medications, it is not explicitly recommended to go back and forth between two pain medications. Switching to a different medication is a clinical decision (previous medication isn’t working, pt not tolerating previous medication, etc.), therefore there should be no reason to revert back to using it after the switch.
Q - Can I use a prefilled saline flush to dilute pain medications?
A - Using prefilled saline flushes is not recommended for mixing medications. It is not a standardized syringe (sticker with markings) and could easily be confused for a flush, potentially causing a significant patient safety event. Labelling of all medications drawn up and/or mixed in syringes is recommended and contributes highly to patient safety.
Q - How important is the Medication Cross-Check when in an emergency?
A - Pain management for our patients is a priority, but not a life saving situation. Take the additional time to complete medication cross checks prior to all medication administrations.
Q - Can you recommend a standard dilution strategy for ketamine?
A - Consider drawing 1ml (50mg) of Ketamine into 10cc syringe and diluting with 9cc of saline. That give 50mg/10ml or 5mg/1ml in the syringe. For a 100kg patient, IV dose of 0.25mg/kg, that would 5cc from the syringe, or 25mg.
Q - Is there a chance a "Better Pressor" is coming in the future?
A - That is currently being worked on provincially (a shock medical directive with potential push dose epi). That said, dopamine is what we have for now and it is still important to be comfortable with the medication and USE it when indicated, as the alternative (no pressor for certain shock states) is worse for the PT.
Read more …Frequently Asked Questions