Newborn Resuscitation and NRP 8th ed. guidelines
Question# 794
Answer:
Firstly, after reviewing the most recent NRP guidelines (8th edition) it was confirmed that positive pressure ventilation (PPV) is conducted for 30 seconds, however in their diagram it states 1 minute total for both the dry, warm, stimulate manoeuvres and PPV with room air. It does appear that the diagram is a bit confusing, however the 30 seconds for each of those manoeuvres is still considered best practice. Recent literature states that most newborns requiring any interventions respond really well to warming and stimulation and then PPV and it is important that each step is carried out in the correct order. Conversely to the studies about PPV working really well, ventilating newborns with 100% oxygen has been associated with worse neurological outcomes.
More specifically, as per the Canadian Pediatric Society, the "golden minute" of NRP 8th ed. refers to the goal to perform an intial assessment of tone/breathing, perform initial steps (warm, dry, stimulate, position airway, suction PRN), and provide PPV within the first minute of resuscitation. Effective PPV resulting in chest movement (i.e. adequate ventilation) should be continued for 30s before reassessment of the HR to determine next steps.
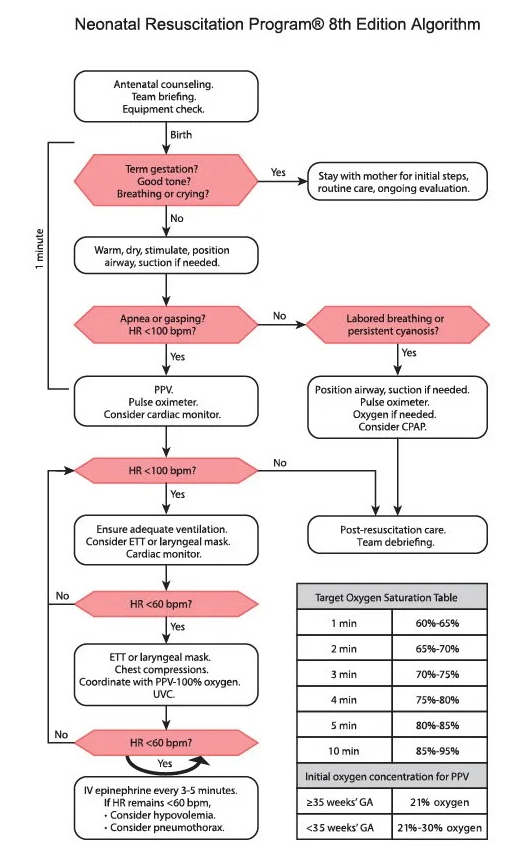
Regarding the Epinephrine, as you mentioned NRP states that a range of 0.01mg/kg-0.03mg/kg of 1:10 000 is appropriate and our current directives state 0.01mg/kg. NRP 8th ed. does introduce an abbreviated initial epinephrine dose of 0.02 mg/kg IV/IO "to enhance educational efficiency", but acknowledges acceptable range is 0.01-0.03 mg/kg. That said, animal research is suggesting high dose (0.03 mg/kg IV/IO followed by 3 mL/kg flush) may improve ROSC so this change may be considered for incorporation into future BH directives pending future research. It is also important to note that there is currently not enough research regarding the best doses of Epinephrine in newborn resuscitation and that is why there still exists a range instead of a prescribed amount. “The current recommendations are extrapolated from adult, animal or manikin studies that do not adequately represent the transitioning circulation and fluid-filled lungs characteristic of newborns” [3].
Regarding the cuffed versus uncuffed tubes, AHA states that cuffed tubes are recommended as they improve capnography accuracy, decrease the risk of aspiration, reduce the need for ET tube changes and improves pressure and tidal volume delivery. As previously mentioned, the cuff can cause airway damage however other studies have shown that it may actually decrease airway trauma by decreasing tube changes as long as inflation is done slowly, and the correct size tube is used. Additionally, the 2020 PALS guidelines have stated the risk of subglottic stenosis and post-extubation stridor is the same between the modern cuffed and uncuffed tubes. To calculate the proper size of a cuffed ETT the formula is Age/4 + 3.5. Consider using 1 ml increments for cuff inflation to help prevent over inflation and subsequent trauma.
We would also just like to highlight the use of the Broselow tape or an RPPEO approved pediatric app such as Pedi STAT if you are ever unsure of medication dosing or ET tube sizing. These reference materials can be a great help on a very busy and challenging newborn resuscitation call. Simply document which reference material you chose to use as there are sometimes small discrepancies between them.
There is also a good podcast, located in MedicLEARN-Elective CME-2022, called "Critical Levels - Critially Ill Children & Organ Donation" that is an additonal reference on this topic.
References
[1]- https://www.ahajournals.org/doi/10.1161/circulationaha.110.971119
[2]- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6132085/#
[3]- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6518253/
[4]- https://publications.aap.org/pediatrics/article/147/Supplement%201/e2020038505E/73495/Part-5-Neonatal-Resuscitation-2020-American-Heart?autologincheck=redirected
[5]-https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7017642/#
[6]- https://www.ahajournals.org/doi/10.1161/CIR.0000000000000901